Vitamin D is a steroid hormone that is obtained through diet or synthesised in the skin from cholesterol when the skin receives adequate sun exposure (the main means of obtaining the vitamin). Unfortunately, exposure to direct sunlight has declined dramatically in today’s society with the increase in the number of office jobs. Furthermore, as we grow older, our ability to absorb vitamin D decreases. Vitamin D deficiency is a global public health problem, affecting all age groups. Recent studies have shown that about 70% of society is deficient in vitamin D1
Endogenous vitamin D synthesis occurs in the skin and is limited to the period of sun exposure. The ultraviolet B rays are able to transform 7-dehydrocholesterol into cholecalciferol (vitamin D3). In order to attain its active form, vitamin D3 undergoes other transformations in the liver (into 25‐hydroxycholecalciferol; calcidiol, which is the most important metabolite of vitamin D3). The next transformation stage occurs in the kidney, where the calcidiol is transformed into the active form of vitamin D3, calcitriol (1,25-dihydroxycholecalciferol). Calcitriol serves as a transcription factor for genes to target proteins and therefore belongs to a wide range of hormones. It is for this reason that vitamin D is considered a prohormone and not a vitamin (Fig. 1).²,³
Soon after the discovery of vitamin D, the relationship between vitamin D and parathyroid hormone was recognised, as well as vitamin D3’s role in the regulation of mineral and bone haemostasis. In this process, the active form of vitamin D, that is, calcitriol, targets different mechanisms to maintain the level of calcium. In addition, it activates bone formation and regeneration, supporting cell differentiation and increasing the serum concentration of calcium and phosphate.4 Studies show that vitamin D stimulates osteoclastic activity and increases extracellular production of the protein matrix by osteoblasts. One of the well-known and early diseases that result from vitamin D deficiency is rickets in children (and osteomalacia in adults), characterised by a serious mineralisation disorder.5 For this reason, many studies have focused on the role of vitamin D in bone health. In addition, vitamin D has gained increasing importance in the treatment of patients suffering from osteoporosis. Vitamin D deficiency is best known and associated with women suffering from osteoporosis and menopause. However, some studies have investigated its significant and substantial role in several other diseases, for example depression, dementia, Alzheimer’s disease, asthma, cancer, cardiovascular disease and diabetes. It is also important to highlight physiological functions, such as muscle strength, neuromuscular coordination and the release of hormones, that are, together with the strengthening of our immune system, impaired by a vitamin D deficit.⁶⁻⁸
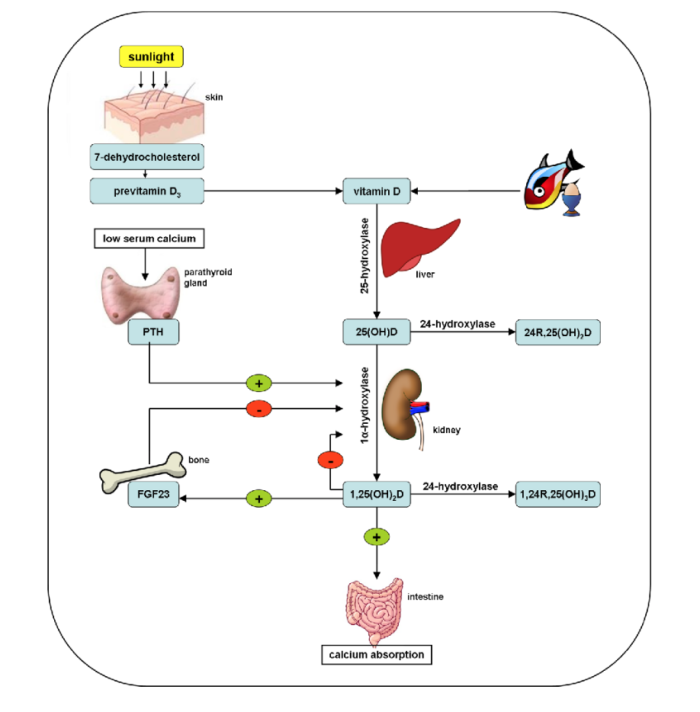
Fig. 1: Schematic image of vitamin D synthesis. PTH = parathyroid hormone; FGF23 = fibroblast growth factor-23; 25(OH)D = calcidiol; 1,25(OH)2D = calcitriol; 24R,25(OH)2D = 24,25-dihydroxycholecalciferol; 1,24R,25-(OH)3D = 1,24,25-trihydroxyvitamin D3. (Image: Dr Stanley)
Over the past decade, several studies have demonstrated the crucial role of vitamin D in general health and its wide range of functions throughout the body.⁴ Several studies have reported the influence of vitamin D in preventing chronic diseases and reducing the prevalence of cardiovascular and metabolic diseases, such as diabetes mellitus.⁶ In addition, many studies have analysed its impact on the immune system, and its ability to reduce inflammation and support regeneration has been demonstrated in different preclinical and clinical studies.⁹ In this context, vitamin D has also shown a beneficial impact in the prevention of infectious bacterial and viral diseases, such as influenza,¹⁰ among other acute respiratory tract infections.¹¹ In addition to the classic role of vitamin D in bone health, it stands out for its important immunological characteristics. More recently, vitamin D deficiency has been associated with an increase in dental implant failure and complications, among others.¹²⁻¹⁹
Optimisation of vitamin D levels before surgery is essential to maximise wound healing. It is essential that levels are optimal, especially in dental medicine, so that the process of osseointegration of dental implants and the integration of bone grafts placed occurs with the greatest success.¹⁴
How to optimise vitamin D levels
Vitamin D (calcidiol) is a highly lipophilic molecule. When the vitamin circulates in the blood, about 80% of the vitamin is linked to its carrier protein (vitamin D-binding protein). Another 10% to 15% of vitamin D is transported by the transport protein albumin. Only a minor part of vitamin D circulates freely in the blood and thus provides greater availability for the cells. The serum concentration of calcidiol is the most reliable indicator of vitamin D levels. However, measuring free calcidiol is technically quite difficult owing to its low concentration and limited availability of test methods.²⁰ Similar to other vitamins and blood components, vitamin D values are expressed mainly in nanomoles per litre (nmol/l) or in nanograms per millilitre (ng/ml) according to the unit system used (1 nmol/l = 0.4 ng/ml; conversion factor: 2.5). There are different recommendations when it comes to reference ranges of vitamin D. A level below 20 ng/ml defines a deficiency. Optimal levels, above 30 ng/ml, are needed to maximise bone health, among other benefits of vitamin D. However, the most often recommended range, considered adequate and healthy, is between 40 and 60 ng/ml.²¹ For individuals undergoing any type of dental procedure, values greater than 40–60 ng/ml are recommended, because after a period of stress (such as dental surgery), levels can decrease substantially.⁶
Unfortunately, our normal diet does not produce sufficient vitamin D levels. Dietary examples are cod liver oil (400–1,000 IU/teaspoon), fresh salmon (600–1,000 IU/100 g, vitamin D3) and dairy (100 IU/85 nmol usually vitamin D3). According to the guidelines of the American Association of Clinical Endocrinologists and the American College of Endocrinology, supplementation is recommended to maintain levels above 30 ng/ml (Table 1).²²
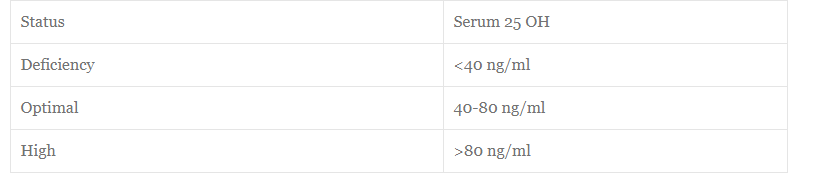
Table 1: Health indicators for various serum vitamin D levels.
Vitamin D plays an important role in supporting the immune system, in integrating various biomaterials, in minimising additional inflammation caused by surgery and in other metabolic processes, such as bone remodelling. For this reason, some complications in dentistry have been related to vitamin D deficiency.
In 2009, a first animal study investigated the role of vitamin D in osseointegration of dental implants.¹⁶ Implants were placed in both normal control animals and those deficient in vitamin D, and were subjected to implant placement and explantation tests, as well as histological analysis. Explantation tests revealed an approximate 66% decrease in value in the vitamin D deficient group and significantly less bone–implant contact as early as 14 days after implant placement. It was concluded from this study that the effect of vitamin D deficiency was significant.
After years of initial preclinical studies demonstrating the marked impact of vitamin D deficiency on osseointegration, additional clinical studies have been published. In 2014, Bryce and MacBeth reported that vitamin D deficiency could be a causative factor in failure of immediate implants.²³
In 2016, Fretwurst et al. observed that the early removal of implants at a university dental clinic was subject to much controversy for possible causes of implant failure: surgical technique, diabetes, smokers.¹³ These randomly chosen implants were often removed just 15 days after placement, and patients were sent for various blood tests. In all cases, serum vitamin D levels were found to be extremely low (< 20 ng/ml). This study group reported that, after a six-month period of supplementation, vitamin D levels increased (> 46 ng/ml) and the implants were successful and were osseointegrated in all cases after adequate supplementation. It was also highlighted that future clinical trials are needed to assess the relationship between vitamin D deficiency and implant failure.
In 2017, Insua et al. wrote an extensive review article on the concept of peri-implant disease being caused by osteoimmunology and bone macrophages and their decomposition and maintenance.¹⁵ A section was dedicated to vitamin D and its correlation with the smaller bone surface in contact with the implant, possible complications and peri-implant bone loss over time. In addition, the immune system was discussed during peri-implant tissue haemostasis/osseointegration.
In 2018, Guido Mangano et al. published a retrospective study in which 1,740 implants were investigated in about 885 patients.¹⁴ To date, this represents the largest study on the subject in which implant failure rates were collected, in addition to other known factors associated with dental implant failure, such as smoking and generalised periodontitis. The conclusions of this study demonstrate the need for vitamin D testing and supplementation before placement and during maintenance after placement of the dental implant.
Vitamin C and antioxidants also play an important role in healing in dentistry
Apart from vitamin D deficiency, several factors can compromise wound healing, such as periodontal disease, poor diet, ageing, diabetes, smoking, excessive alcohol consumption, and stress.²⁴–²⁶, ²⁷. Oxidative stress is considered to be one of the main causes of tissue degeneration and chronic wounds that do not heal.²⁸, ²⁹ To combat oxidative stress, every cell in the body requires molecules known as “antioxidants”, which prevent tissue damage.³⁰
Unfortunately, a large percentage of the population today suffers from vitamin and mineral deficiencies directly linked to antioxidant levels. For optimal wound healing, patient’s antioxidant levels must be increased before surgery. Vitamin C is one of the vitamins that is considered important owing to its antioxidant, collagen synthesis and immunity functions.³¹, ³² Other important compounds for optimal wound healing include flavonoids,³³ the vitamin B complex,³⁴ carotenoids (vitamin A), magnesium,³⁵, ³⁶ zinc,³⁷ manganese and selenium.
Unfortunately, a large percentage of the population today suffers from vitamin and mineral deficiencies directly linked to antioxidant levels. For optimal wound healing, patient’s antioxidant levels must be increased before surgery.
The role of vitamin D in infectious diseases
The immunomodulatory function of vitamin D and its impact on the immune system reflect its potential role in the defence against infectious diseases. For this reason, there has been a growing interest in the influence of vitamin D levels on the prevalence and incidence of infectious diseases.³⁸–⁷⁵ Its potential anti-infective capacity has made vitamin D a favourable candidate for adjuvant therapy in treating numerous infectious diseases. A systematic review highlighted the correlation between vitamin D deficiency and the status of patients with chronic hepatitis B.⁴⁴ In addition, it has been shown that a low level of vitamin D is associated with a high viral load of hepatitis B. Another study showed that genetic variants in the metabolic pathway of vitamin D are involved in hepatitis C virus infection.⁷⁶ More recent research suggests that vitamin D may inhibit herpes infection in oral epithelial cells, regulating the gene expression of defence molecules such as interleukin-37.⁷⁷ Some studies have also revealed the preventive impact, already mentioned, of vitamin D supplementation in reducing infections caused by influenza in childhood.⁵⁴ In addition, several studies have highlighted the positive impact of vitamin D on patients infected with HIV-1.⁷⁸ Other studies have suggested that micro-RNAs regulated by vitamin D may have a protective impact on dengue virus infection.⁷⁹, ⁸⁰
Another study showed that patients who developed pneumonia had a much lower level of vitamin D than the healthy group did.⁸¹ Interestingly, the vitamin D receptor polymorphism was questioned in a recent meta-analysis for its correlation with the risk of viral infections.⁸² Based on this data, a recently published review investigated the potential role of vitamin D in SARS-CoV-2 infection, as this virus also belongs to the family of encapsulated viruses.⁴³
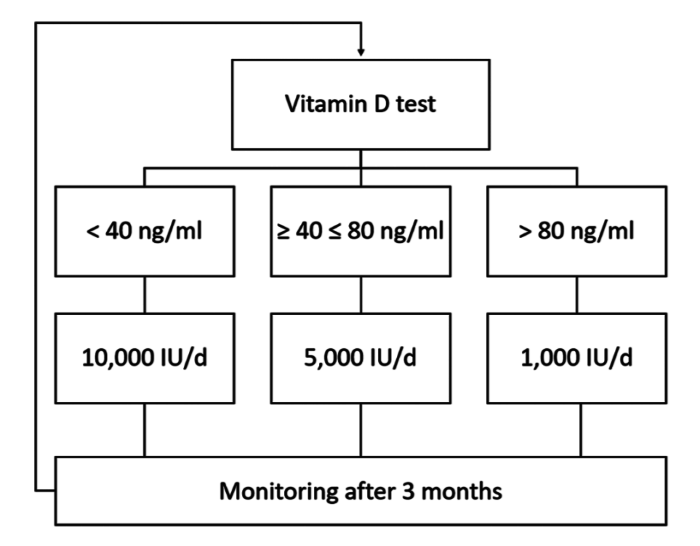
Fig. 2: Supplementation protocol of vitamin D for adults developed by Shahram Ghanaati.
Conclusion
Vitamin D deficiency remains one of the most prevalent vitamin deficiencies, and it is directly related to bone remodelling, as has been reported in the literature. It is important to highlight that vitamin D is also related to the immune system, mostly when biomaterials are placed in the bone, such as grafts and dental implants. This article highlights that recent studies have shown a significant additional increase in early dental implant failure when vitamin D levels are low and that vitamin D is a potential aid in resisting the spread of infectious diseases like COVID-19. Furthermore, this article has demonstrated the recommended doses of vitamin D depending on the vitamin D level results.
About the authors
Dr Miguel Stanley is the clinical director of White Clinic in Lisbon in Portugal.
Dr Ana Paz heads the scientific research and development department at White Clinic.
Prof. Shahram Ghanaati is senior physician and deputy director of the clinic for oral, cranio-maxillofacial and facial plastic surgery at the Goethe University medical centre in Frankfurt in Germany and head of the FORM-Lab research laboratory, also at the medical centre.
Editorial note: A list of references is available from the publisher.