After the French dentist Pierre Fauchard, who is credited with inventing modern orthodontics, first published his pioneering book in 1728 on dental treatments, in which he explained how to use a Bandeau device, a horseshoeshaped piece of iron that helped expand the palate, people figured out that they could improve facial anatomy and the position of the teeth and consequently improve chewing, posture and ultimately facial aesthetics, by applying mechanical forces to teeth. This made it something desirable and, to a certain extent, a consumer product.
There are so many different ways to do this nowadays, so much has been discussed, analysed and proved to be true, and by the same token, we all have come to understand that many things that we were doing in the past no longer make sense. I am certain that we have all seen historic images of external devices applying mechanical forces that look like something out of a Tim Burton movie. It is strange to think that in the past people would be open to use of such dramatic orthodontic devices in order to achieve a better smile.
We have come a long way just in the past 20 years. I graduated in 1998, and I never really got into orthodontics as a practitioner, but very early on understood its importance in my clinic. I am proud to say that I have been working alongside a fantastic orthodontist since the very beginning, for almost 20 years now. Back in the day, we used classic brackets with elastics, and I always paid a lot of attention to how much art, planning and strategic thinking went into diagnosing each case. Early on, in 2003, we acquired a digital panoramic radiography unit that could also take cephalometric radiographs to enable proper cephalometric planning. The investments in appropriate technologies have not stopped since. As an implant surgeon and prosthodontist, I had the right team and tools to head bravely into the new century. I am very happy to say that, with solid foundations in science and clinical evidence and the right mentors, for over 20 years we have been doing interdisciplinary case management and pre-surgical orthodontic treatment, combining orthodontics and implant treatment in complex cases, to then finally restore a case to perfect occlusion when necessary. Little did I know back then that this would be the right way to do things 20 years later and ubiquitously accepted.
Today, thanks to concepts such as digital smile design (DSD) and special software and 3D printers, we can very easily understand where we need to take the dentition with orthodontic movements prior to minimally invasive treatment with veneers, just as an example. Back then, this required quite a lot of thinking and a very hands-on approach. I feel I have acquired knowledge as the founder and clinical director of an interdisciplinary clinic to talk about orthodontics and aligners.
I very clearly remember the excitement when we discovered the Damon system, which used self-ligating brackets that were gentler on teeth and soft tissue and that required a lot less force to move teeth with much higher efficiency and in fewer appointments. Dr Alessandra Curto, head orthodontist at the practice, took a course on the system and we immediately implemented the system at the White Clinic. Despite the cost of the system, we quickly understood the implicit benefits of having a system that was faster, required less management and was ultimately more comfortable for our patients. Obviously, we passed on that extra cost to the patient, and yes, it was a harder sell back then; Portugal was and still is, after all, the second or third poorest economy in the European Union, but our ethos has always been nothing but the best for our patients. It is important to say that we have absolutely no commercial relationship with Damon system and never have had. I just always believe good things deserve a mention. We still use this system today and have done some amazing cases over the years that we believe could still not be done with aligners, although the things we can do with aligners is increasingly improving. It is important to say that my team and I have always practised Slow Dentistry and spend on average 2.5 hours planning each case prior to starting therapy and follow the No Half Smiles treatment philosophy, which I created in 2006. This philosophy basically means that we never treat just one arch, or perform partial dentistry, leaving untreated teeth in the oral cavity. The aim is to always restore the whole mouth to health, function and, if so desired, aesthetics. Patients with few problems have fast treatment times and little work is necessary, and those with major issues need a lot more work, time, patience and care and their treatment ends up costing a lot more too. No matter what, we always focus on establishing good occlusion and biology, as aesthetics can usually only be achieved after these parameters have been set. It is also worth mentioning that the White Clinic has never had investors or shareholders, is not part of a dental service organisation (DSO), or had never worked with an insurance company. We also have never sold courses or distributed dental products. Why am I saying this? Well because we can focus all our time and our resources on investing in technology, training and doing the right thing always. I am not saying that these are wrong, just that we prefer to focus on the patient and on what truly matters, doing extraordinary dentistry every day and updating knowledge and technology as it comes into existence, so we are always ahead of the game, offering our patients the best there is to offer in any given year.
When in 2005 we were introduced to clear aligners from Align Technology, I was truly blown away. I mean 3D printing was unheard of in real life; it was a thing of sci-fi. I love exciting new technologies that offer more and are better for our patients. Remember, in 2005 there was no social media and no real way of seeing what the world was saying about anything. We started using aligners immediately, and I can tell you that it was not an easy sell to patients, mostly because of the cost. Notwithstanding, we pushed on, and I recall that sales represented about 5% in the first year. Few dentists in Portugal were using clear aligners, and it was really difficult to gain credibility for this modality, as there were no social benchmarks.

Fig. 2: Large gaps between the teeth caused by poor orthodontic planning.

Fig. 3: Large gaps between the teeth caused by poor orthodontic planning.
Patients had no way of knowing what they were like, asking friends and family, as no one was really using aligners back then and no big marketing was being done, so we really had to spend hours of our time explaining to patients what they were and the implicit benefits over traditional fixed appliances, which include the following:
- easier to floss and brush teeth;
- more aesthetic;
- better for people with public-facing jobs that require them to talk, model or act, for example, and for high-performance athletes;
- ability to eat one’s favourite sticky foods;
- more control over the planning and better visualization of the final result;
- possibility of refinement at the end; just to give a few examples.
In many cases, we had patients wanting aligners, but the traditional method was better, and vice versa. We would only do what was best for the patient.
I did some TV shows on prime-time TV, performing interdisciplinary dentistry, and to the best of my knowledge, it was the very first time in the world that a TV show used dental implants as part of a smile makeover. Unfortunately, orthodontic treatment was not included, but it was an incredible opportunity to show the country the difference between single-tooth traditional quick-fix dentistry and full-arch smile restorative treatment. As a result, the White Clinic became a household name in dentistry and a benchmark in the country for excellence in oral care. This obviously made communicating complex treatment and products such as clear aligners a lot easier, and as the years went by, aligners became more ubiquitous in our major cases, including complex ones. We performed increasingly more pre-veneer orthodontic cases, and consequently our confidence levels in the technology grew and I would say that by 2009/2010 they represented 50–60% of our orthodontic cases.
As clinical director, my job has always been to implement new strategies, technologies and techniques and to ensure that we have the time to implement things into our workflow and ensure that whatever we do has the patient’s best interests as the primary focus. This means that we always incorporate anything that will make the workflow and outcome faster, better and, if possible, more affordable for the patient. This last objective has not really always been possible, as employing new technologies usually involves more investment, time and training and expensive materials. I was very fortunate early on in my career to start lecturing around the world, mostly on implant dentistry, but since I am also a cosmetic prosthodontist, I spent a lot of time showing the audience and my colleagues these orthodontic cases that we were treating that were all, by default, interdisciplinary in their planning and execution, the final focus always being on occlusion. Biology is “king” at the White Clinic, and for this reason, we acquired the very first full field of view digital CBCT unit in the country in 2008. This specific one allowed us to stitch the DICOM files together, enabling our team to see the skull in all its glory in a beautiful 3D image.
I have to say that the initial premise of acquiring CBCT technology was to improve our planning for dental implants, at the time the most complex part of the practice. However, we very quickly understood the implications this technology could have for improving treatment for orthodontic patients who had complex biotypes or required complex movements. Being able to complement the cephalometric analysis, done with traditional 2D images from a panoramic and tele-radiographic unit, was quite groundbreaking. We were able to instantly see the tooth–bone ratio without any of the soft tissue and to use the software to rotate the skull and understand immediately the challenges that we would face in applying complex orthodontic movements—revolutionary! This is something we started doing daily in our practice back in 2008, when only 1% of dental practices globally had CBCT technology, according to major manufacturers.
Armed with this new imaging capability, we grew our orthodontic department exponentially. To the credit of Dr Curto, in 20 years of working together, we have never had one case of root resorption and, in the roughly 5,000 cases performed together, perhaps no more than ten instances of minor gingival retraction. These were primarily due to the patients’ thin biotype and the risk was explained to these patients prior to initiating the treatment; therefore, we were not surprised when it occurred and we were able to restore the gingiva with minor gingival grafting by our periodontics department.
I have set all this out to demonstrate that we really take treatment planning seriously. It takes time. Those of you who work with aligners know the importance of entering the right information into the software through the aligner provider’s platforms to then work with the company to ensure that the treatment is the best possible for the patient.
If we did a global survey right now on the average time that dentists spend on planning with the software for their aligner cases, what do you think the answer would be? What is the ideal time that an orthodontist or general practitioner should spend interacting on the cloud software to ensure the safest biological movement possible? Obviously, the more complex the case, the more planning must be done, or so the consumer or other dentists might be led to believe!
“As I progress in my career, I am learning more about the dark side of dentistry”
Dr Miguel Stanley
As I progress in my career, I am learning more about the dark side of dentistry and of growth strategies that clinicians and corporations have that very rarely have the patient’s best interests at heart. There seems to be many instances of corruption of care in which I would presume the patient trusted the dentist to give him or her the best care and believed that the Hippocratic oath of do no harm was being applied throughout the entire procedure. This was so much easier to control when it was the dentist directly applying the brackets and arch wires and bending them to apply micro-forces throughout the orthodontic treatment with the traditional method. There was no interface, no outsourcing of planning and no third party, and if things went wrong, the dentist had to “face the music”. He or she was the person in charge and could not shift the blame of poor outcome to anyone else. Obviously, we would still see some cases of simple orthodontic treatments taking much longer than they should have, the business plan of the dentist being to have constant income from a large multitude of patients.
I believe that this is one of the upsides of aligners, as there is a clear end date built into the system. I have seen hundreds of cases over the years of patients who have had their mouths ruined by orthodontists who seemed to completely forget or overlook the inflamed gingivae and carious lesions in the four to five years in which they were straightening their teenager patients’ teeth. Obviously aligners actually changed the game in more ways than one. We now have the opportunity to outsource planning and have an end date in mind at the very beginning of the procedure. This is fantastic! However, like all software and even any artificial intelligence, also used in orthodontic planning nowadays, it is all about who programs the software and what the ethos of that planning is. This means that the better the information given to the software is, the better the engineers or technology can design the case. Even today, most orthodontic aligner cases require the dentist to interact with the providing company to fine tune the treatment proposed. It is obviously utopia to believe that everybody does it properly. As the founder of the Slow Dentistry Global Network, which focuses on seeing fewer patients a day in order to provide a higher degree of care, safety, hygiene and treatment planning, I have never worked any other way and I am well aware that there are many dentists around the globe who do take the appropriate amount of time to put proper thought into planning cases and aligners and interact more than once with the providing companies, suggesting many alterations based on their intimate understanding of the patient’s mechanics and physiology.
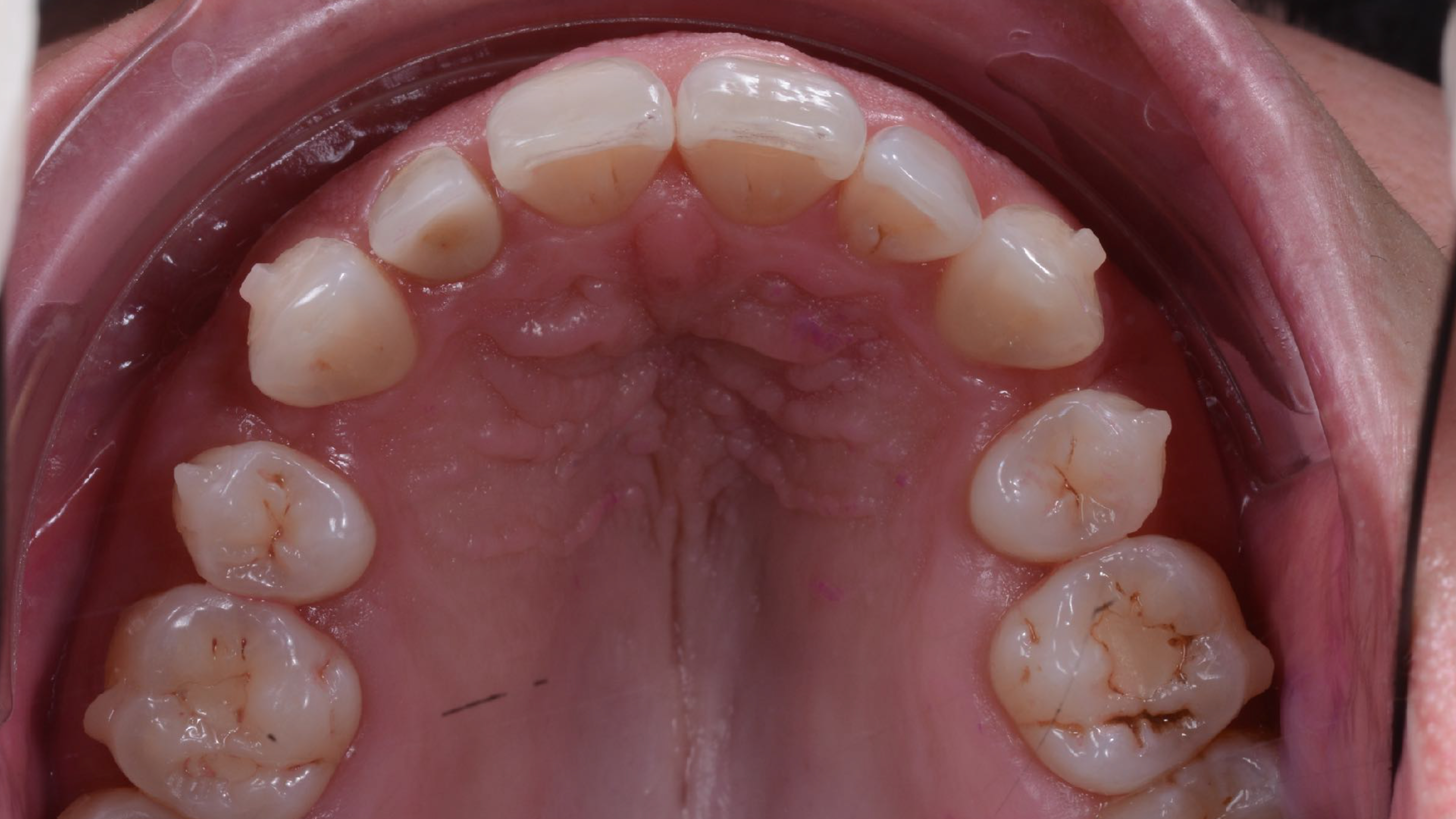
Fig. 4: Before beginning the 18-month retreatment.

Fig. 5a: After an 18-month treatment to open space, driven this time by design, …

Fig. 5b: …and after implant and final ceramic restorations.
“Would it not make more sense to reward dentists based on quality of outcome instead of volume of sales?”
Dr Miguel Stanley
But let us face it, can we really believe that companies that are listed on stock exchanges and have a duty to their shareholders to generate as much profit as possible really care about dentists who take extra time in carefully planning their cases? Do they prefer practitioners who sell the largest number of cases as possible? This is a very important question. As I see it, if we look at the way things are being done currently, we have some systems that are rewarding dentists with such accolades as “platinum” and “diamond” provider recognition, implying that these clinicians must be better providers than those who are simply bronze or silver providers. Why would a potential patient seeking aligner treatment choose a provider who appears to be less than the best? Moreover, we all know, or should know, that many of these reward systems also allow the providers to pay less per case if they sell more cases—this is a massive financial incentive to sell as many cases a year as possible. Why? Recognition as a platinum or diamond provider is not only cheaper and more profitable, but also creates the illusion in the marketplace that the provider is a better dentist. This is simply not the case in general.
I think we need to have an open discussion about this. Would it not make more sense to reward dentists based on quality of outcome instead of volume of sales? Do you not think that the consumer would prefer to have a dentist whose final results are almost always identical to the initial treatment plan discussed with the provider, whose final scans are very close or identical to the treatment plan, or who achieves results with no root resorption or gingival recession and within the time frame established? I think that these are the orthodontists who should receive accolades and global recognition for being the best of the best! What we have is pure capitalism disguised carefully as great healthcare. Is this really the best we can do in 2022?
Do not get me wrong: I am all for being profitable, but it should never be at the expense of the patient’s trust. Trust is the foundation of any medical relationship. If we are selling patients the fact that we are better than our peers because we have received such accolades, then we need to be open about exactly what those accolades are and commit to improving our ecosystem.

Fig. 6: 3D-printed mock-up and index tray to test the new design.
I think that dentists who take more time to plan cases, use CBCT and intra-oral scanning technology, and carefully integrate orthodontics with periodontics and restorative dentistry start any case with a DSD study, in order to understand whether the tooth ratio is ideal for the patient’s face. This is also something most aligner companies overlook, focusing only on straightening the arch and bringing the occlusion ideally to a Class I occlusion, often overlooking the fact that the teeth might be too small for the patient’s mouth. I have seen this happen so many times. Treatment seems to be going well, but at the end of such a long journey, the patient is unhappy with the results, because he or she does not really understand that the problem involved the shape and size of the teeth too and not just misalignment. This should not be happening in 2022. We have the tools and resources to understand all of this, before we even touch the patient’s anatomy.
Would it not make more sense to let the patient know prior to initiating a long orthodontic treatment that at the end of the procedure he or she might need to undergo some crown lengthening and/or veneers? People have a right to know before they decide to proceed with alignment that they will have to incur extra costs and undergo more therapy to achieve the desired results. This is all possible with digital software and can be outsourced just like the aligners. I believe that groundbreaking technologies such as those employed by DSD, deserve all the respect and recognition, as these promote and enable the ideal of designing the smile prior to treatment, and this is critical to understanding what is necessary throughout the entire treatment (I have no commercial relationship with DSD–I am just a fan). We were doing it long before the technology existed; it just took a lot longer. Many dentists were doing this, but now, more can do it. It appears, however, that way too many dentists are too cheap or too lazy to invest time and money or, even worse, are scared that the extra costs will scare patients away.
Success is a mindset!
Having an intra-oral scanner and a CBCT unit and using the cloud and even outsourcing planning only makes life easier, but you have to have the moral compass to make certain that you are always putting your patient’s biology first and not your pocket just so that you can jump category, obtain more rewards and be recognised as the leader in your community to outshine your competition. This is not a race. You should only consider yourself a leader when all your cases are delivered with the best intentions possible and the best results consistently.
Recently, I gave a lecture in Como in Italy for the Digital Dentistry Society, of which I am the vice president. I presented only one case: the case of a 44-year old woman with no financial limitations who went to a very good orthodontist in my country to have aligner treatment. After two years of treatment, she could not close her mouth properly, had massive gaps between her teeth and was suffering from tension headaches and temporomandibular joint issues as a direct result of her treatment. She was desperately trying to find out what was going wrong and why her aligners were not offering her the solutions that she was sold in the beginning. I am sad to report that the dentist in question extracted two healthy premolars because, I presume, the software told him to do so. I can only speculate that no CBCT scan or DSD or even thought process went into the treatment planning for this patient, who lost not only her smile but also her trust in dentists. After careful discussion with my team, looking at the CBCT scan and conducting a DSD, we quickly understood that the tooth ratio was too small for her face. Her premolars should not have been extracted. If anything, she needed her arch expanded to improve her airway, and at the end of her orthodontic treatment, she needed a vertical dimension augmentation via full-contour veneers. We printed a 3D mock-up for her, and she was brought to tears seeing photographs and herself in the mirror and finally understood what was possible with a proper plan.
We spent a lot of time helping her understand why things went wrong and what we could do to improve the situation. It took us two years to reposition the teeth, to open the gap created by this orthodontic mismanagement and to finally place implants where her premolars had been, establishing her smile and function. She is the most grateful patient today and has had her trust and not just her smile restored. She is a very communicative patient and refers a lot of work. We are grateful.

Figs. 7a & b: Comparison of (left) the initial situation with the final result with full-contour veneers, implants and a new vertical dimension after the aligner treatment.
I believe that the reason this happens in the first place is that the largest clear aligner companies in the world seem to be focused on profit and take very little responsibility for quality control regarding the final use of their product. It is very easy for them to say that it is the dentists’ responsibility at the end of the day to do the right thing. They are right, but not all dentists have the right training, tools or mindset. We need more quality control to benefit the patient.
Rewarding dentists on volume of sales and not quality of outcome creates an environment for absolute corruption of care in my opinion. Some dentists might not like what I have to say, but I am sure that the patient, who is the real consumer at the end of the day, would prefer to know the facts. I believe soon the interface will be more public facing and patients will have access to this information. Times are changing; we must change with them. The technology that was invented back in the nineties using 3D printing and stereolithographic technology and software to straighten teeth was absolutely incredible. It is now available ubiquitously around the world, many companies providing what appears to be the same thing.
I personally will always prefer to work with companies that can integrate CBCT data with intra-oral scan data, we are already using such systems that have a higher degree of monitoring of treatment planning. I would also love to see them offering rewards on the quality of outcome, based on the final CBCT and intra oral scans sent back, comparing the results with the treatment planning. I do not think that exists yet, but I have heard that some companies are working on this, and that is the way it should be done! Unfortunately, I have come to understand, after 24 years in dentistry and having lectured in more than 54 countries around the globe, that owing to global economics not every dentist can place ethics at the centre of their treatment all the time. They often lack the resources to do the right thing and are trapped in the past. It is the obligation of large companies to ensure some oversight in the technology to make sure that the patient, who is the real consumer, receives nothing but the best. Hopefully artificial intelligence will mitigate these concerns in the future, and I am certain that we are all heading in the same direction: great volume of sales and extraordinary quality of care.